Breaking Up With Meditech

“It’s not you, Meditech, it’s me.” The words almost catch in your throat as you tentatively reach across the table, taking their hand in yours for what you know will be the last time. Your eyes search theirs for any signals of emotion, any glimmer into how they are taking the news, but they seem distant and you continue: “I’ve met someone…they’ve acquired me…my heart.” Still no signs of emotion, but they look ponderous as if the information is slowly cohering into understanding. After a moment, they pull their hand away from yours and finally make eye contact and ask, “So can we close out some of these tasks then?”
I’ve worked with a number of hospital systems now that have been acquired by a larger system prior to my contract and bring me on for some version of legacy support/data dumps/getting-the-house-in-order tasks that need to happen so maybe someday in the near or distant future they can make a decision to finally move to a system-wide EHR which may or may not be one that they currently use. The hospital industry is continuing to go through a consolidation trend as is evidenced by this graph from a report put out by the American Hospital Association:
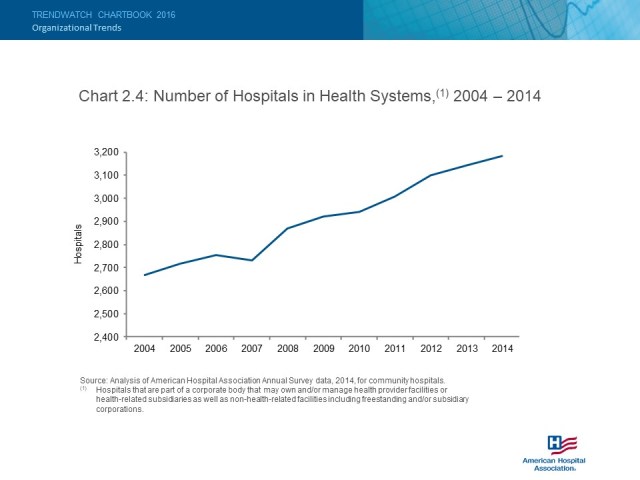 Actually, that type of chart doesn’t really show the trend they were trying to show, but whatever, I fixed it for them:
Actually, that type of chart doesn’t really show the trend they were trying to show, but whatever, I fixed it for them:
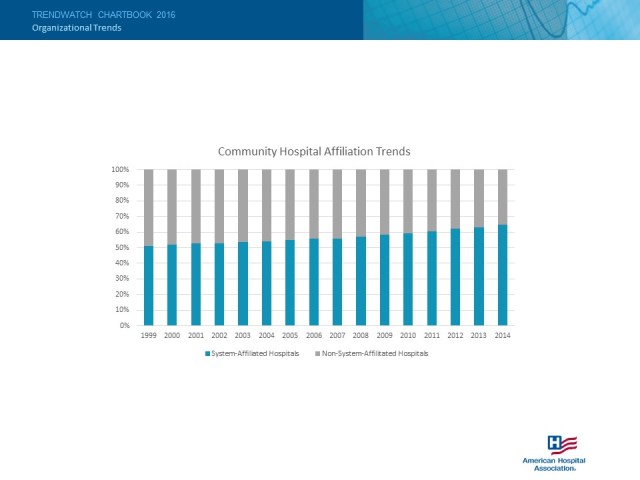
A chart showing a single trend line of the percentage of System-Affiliated hospitals would have worked too, but I’m digressing again.
The point is that Meditech’s industry market share has been predominantly composed of smaller to medium-sized hospitals for the hospital side of their product offerings and then a fraction of that was composed of clinics using the practice management side of their product offerings. These smaller to medium-sized hospitals are the ones being acquired and absorbed into larger systems and those larger systems generally use Epic or Cerner. While diversity is usually encouraged in an ecosystem, any diversity in EHRs that are being use throughout a hospital system is generally detrimental to productivity, efficiency, costs, etc. and therefore, the EHRs of the absorbed hospital systems will be phased out and replaced. Math and deductive reasoning shows us that this means Meditech is losing market share.
Transitioning a hospital and its related clinics from one EHR to another is no simple task, but it’s also not an insurmountable one either. In fact, it’s being done at an increasing rate. Of those that I have been a part of, there seem to be a common list of goals that are initially touted that are either not feasible or perhaps not technically possible in today’s limited interoperability environment so let’s disabuse those now:
Wish list item 1: Auto-loading of patient information from the old EHR to the new EHR
Probability of success: Not going to happen
Issues: Even if you only had hopes of porting a fraction of patient information over, the path to get to a point where that could actually happen is to fraught with complications and a severe hike in project expenses where you should probably just drop this item from your project goals list outright. The reasoning behind this is simply that there is no standard patient file format that exists between EHRs. The very best possible option that is currently available is utilizing CCDs which are required by Meaningful Use to not only be exported from an EHR, but also consumed by them as well. However, in the Meditech world, there is not a mass-export option of CCDs so a manual effort is needed to export these patient by patient. Additionally, there is now an added security risk by saving these CCD files on a server within your organization. Sadly, the “best” option usually turns out to be the same one utilized for a move from paper records to your first EHR: Manual entry of the important data points and forget about the rest.
Wish list item 2: Higher user satisfaction of the new EHR than the old one.
Probability of success: Actually possible
Issues: Just in terms of usability, most users find they take a small step up when moving from Meditech to Cerner or Epic. However, at the same time, everyone hates change. Therefore, before beginning the move to the new EHR it is best to address any process flow differences that exist between offices. By standardizing as many processes as you can on the old EHR, most of the hatred is directed toward the old EHR and the new EHR, which is already set up to accommodate your organization-wide standard processes seems like a huge improvement. It is a bad idea to try and change the processes and workflows of staff in addition to throwing the challenges of learning a new EHR on them. You already did this once when first implementing an EHR, why do it again?
Wish list item 3: Accurate and consolidated financial reporting during the transition
Probability of success: Possible, but resource intensive
Issues: If you don’t already have reporting that you feel is accurate and consolidated with multiple EHRs, you might as well forget about this one until the transition is complete. Unfortunately, the task is generally not as simple as combining the numbers from one EHR with another. Varying process workflows and accounting methods between systems prohibit this from being an accurate way to produce reporting unless you work through those differences.
Wish list item 3: Skipping the whole EHR consolidation thing and maintaining multiple EHRs across the enterprise.
Probability of success: Not in your lifetime, bub.
Issues: Google “EHR interoperability”.
